

Reasonable and Necessary Under the NDIS: What Clinicians Need to Know
Understand the NDIS reasonable and necessary criteria and learn how to write reports that justify supports clearly, specifically, and effectively.
Why "reasonable and necessary" is the concept every clinician working with the NDIS needs to understand
The National Disability Insurance Scheme funds supports for eligible Australians with permanent and significant disability. But not every support a clinician recommends will be funded. The NDIS uses a specific legal and policy framework to decide what gets approved — and the phrase at the centre of that framework is "reasonable and necessary."
If you write NDIS reports, provide therapy for NDIS participants, or support clients through plan reviews, understanding what reasonable and necessary means in practice is not optional. It determines whether your recommendations translate into funded supports, or get rejected on the grounds of insufficient justification.
This post explains the reasonable and necessary ndis criteria in plain language, shows how to apply them in clinical reports, and provides practical wording examples you can use in your own documentation.
What does "reasonable and necessary" mean under the NDIS?
The term "reasonable and necessary" comes from the National Disability Insurance Scheme Act 2013. Section 34 of the Act sets out the criteria a support must meet before the NDIA will fund it.
In plain terms, a support is considered reasonable and necessary if it is related to a participant's disability, is an appropriate use of NDIS funding, is likely to be effective, and does not replace something that should be funded elsewhere — by family, community, or another government system like Medicare or education.
The purpose of this framework is to ensure NDIS funding goes toward supports that genuinely help participants build capacity, reduce their reliance on paid support over time, or maintain their current level of function where decline is otherwise expected.
Clinicians sometimes treat "reasonable and necessary" as a bureaucratic hurdle. It is more useful to treat it as a clinical framework. If you can explain how a support meets each criterion, you are already writing a stronger report.
The core criteria explained
The NDIS Act sets out five main criteria. A support should meet all of them to be considered reasonable and necessary. Here is what each one means in practice.
1. Related to the participant's disability
The support must be directly connected to the functional impact of the participant's disability. It cannot be something that would be needed regardless of whether the person had a disability.
In practice: A participant with autism spectrum disorder experiences significant difficulties regulating sensory input in shared environments, which affects their ability to attend community activities. Occupational therapy to assess sensory processing and develop a regulation plan is directly related to this functional impact.
A general gym membership, by contrast, is not — even if exercise is beneficial — because it would be needed regardless of the disability.
2. Value for money
The support must represent a reasonable use of NDIS funding relative to its expected benefit. This does not mean the cheapest option. It means the cost is proportionate to the expected outcome for the participant.
In practice: Recommending 52 sessions of individual therapy per year for a participant with mild functional impact will likely be queried. Recommending 20 sessions with a clear plan for skill development, review, and transition to lower-intensity support is easier to justify on value grounds.
Clinicians can strengthen value arguments by linking the cost of the support to the cost of not providing it — for example, reduced hospitalisation, reduced carer burden, or maintained capacity for employment or education.
3. Likely to be effective and beneficial
There must be a reasonable basis for believing the support will make a positive difference for this specific participant. This does not require a randomised controlled trial, but it does require more than assumption.
In practice: Citing relevant evidence for the approach you are recommending, noting the participant's history of response to similar supports, and being specific about the expected benefit for this person all strengthen this criterion.
Vague statements such as "therapy will be beneficial" do not satisfy this requirement. Specific statements such as "the participant has demonstrated response to cognitive behavioural approaches in previous intervention, and structured CBT is expected to reduce avoidance behaviour and support return to education within the current plan period" are far more defensible.
4. Takes into account informal supports
The NDIS is not designed to fund everything. It expects that some level of support will come from family, friends, or community networks — what the scheme calls "informal supports." A support request is stronger when it is clear that informal supports are already being used and that the gap being funded is specific and genuine.
In practice: This does not mean clinicians need to prove that a family is exhausted before recommending funded support. It means being clear about what informal supports exist, what their limits are, and why the recommended funded support fills a gap that informal supports cannot reasonably fill.
For example: "The participant's parents provide significant support with daily routines. However, they do not have the training to implement a structured positive behaviour support plan, and the complexity of the participant's behaviours of concern requires specialist input."
5. Most appropriately funded by the NDIS
This criterion asks whether the NDIS is the right system to fund this support, or whether it falls more appropriately under another system — Medicare, state health, education, or aged care.
In practice: This is where many therapy recommendations run into difficulty. If a support could reasonably be accessed through Medicare Mental Health Care Plans, a planner may question whether it is most appropriately funded by the NDIS. Clinicians should be clear about why NDIS funding is appropriate for the participant's specific situation.
Common justifications include: the participant requires a level of frequency or intensity that Medicare plans do not support, the goals of intervention are disability-specific rather than mental-health-specific, or the participant has already accessed Medicare supports and requires additional capacity.

Translating policy into clinical practice
Most clinicians understand the reasonable and necessary concept in principle. The challenge is translating it into the language of reports.
The most common mistake is writing about diagnoses rather than function. A diagnosis does not fund a support — functional impact does. The question a planner is asking is not "does this person have autism?" but "what does this person need funded support to do that they currently cannot do because of their disability?"
A second common mistake is making recommendations without justification. Listing therapy hours or support categories without explaining why that specific volume, at that frequency, for those goals, is both effective and necessary leaves the decision-maker with no basis for approval.
A third mistake is writing for clinical audiences rather than planning audiences. NDIS reports are read by people who may not have clinical training. The clearer and more specific the reasoning, the less room there is for misinterpretation or rejection.
When reviewing your own reports, it is worth applying the reasonable and necessary criteria as a checklist. For each recommendation, ask yourself: Have I linked this to the participant's disability? Have I justified the volume and frequency? Have I cited evidence for the approach? Have I acknowledged informal supports and their limits? Have I explained why NDIS is the right funding source?
Example wording for NDIS reports
The following examples show how the reasonable and necessary criteria can be reflected in clinical report language.
Functional impact statement:
"Due to significant difficulties with emotional regulation arising from his autism spectrum disorder, [participant] is currently unable to maintain part-time employment without regular meltdown episodes that result in dismissal. He requires structured support to develop regulation strategies specific to workplace environments."
Justification for therapy supports:
"Speech pathology intervention is recommended at a frequency of one session per fortnight over 12 months to address the participant's functional communication barriers, which significantly limit her ability to participate in education and community activities. This frequency is based on the complexity of the participant's needs, her history of slow skill acquisition, and the need for regular parent coaching to support generalisation of skills across settings."
Risk-based reasoning:
"Without funded behaviour support, the risk of [participant] engaging in self-injurious behaviour that results in injury or hospitalisation is assessed as high. Current informal supports are insufficient to implement the level of environmental modification and behaviour-specific intervention required to reduce this risk."
Linking to goals:
"A core goal for [participant] in this plan period is to increase independent access to her local community. Occupational therapy is recommended to conduct an environmental assessment, develop a structured community access plan, and train support workers in the implementation of that plan. This support is directly linked to the participant's stated goal and is expected to reduce reliance on 1:1 support for community access within 12 months."
Justifying NDIS funding over Medicare:
"While the participant has previously accessed psychology support under a Mental Health Care Plan, the current intervention goals are disability-specific and focus on functional skill development rather than mental health treatment. The frequency required to support skill acquisition exceeds what is available under Medicare, and the intervention falls within the scope of NDIS Capacity Building — Daily Activities."
Common pitfalls to avoid
Overly emotional language. Statements like "this family is struggling deeply" or "without this support, the participant will suffer significantly" are not sufficient justification. Planners need functional evidence, not emotional framing.
Diagnosis without functional link. Writing "the participant has ADHD and requires occupational therapy" is not enough. The report needs to explain what specific functional limitations arise from that diagnosis, and how occupational therapy will address them.
Generic recommendations. Recommending "therapy support" without specifying the type, frequency, duration, and goals leaves too much room for a planner to reject or underfund the request.
Assuming the planner has clinical knowledge. Write as if the reader has no psychology, OT, or speech pathology training. Every claim that a support is necessary should be self-contained and legible to a non-clinician.
Neglecting to state expected outcomes. NDIS planning is outcomes-focused. Reports that describe problems without articulating what funded support is expected to achieve are harder to approve.

Practical tips for writing NDIS reports that hold up
Be specific about function. Name the activities the participant cannot do, the environments in which limitations occur, and the frequency and severity of the impact.
Use measurable language. Where possible, quantify functional impact. "The participant is unable to attend school for more than two days per week due to anxiety-related avoidance" is more useful than "the participant finds school difficult."
Align recommendations with participant goals. The NDIS plans are goals-driven. Each recommendation should clearly connect to at least one of the participant's stated goals.
Justify volume, not just type. It is not enough to recommend occupational therapy. You need to explain why 20 sessions rather than 10, why fortnightly rather than monthly, and what the plan is for reviewing or transitioning out of that support.
Acknowledge capacity-building intent. The NDIS prefers supports that build independence over time. Where possible, describe how the support is designed to reduce reliance on funded services — not increase it.
Reference relevant evidence. You do not need to cite academic literature in every report. But noting that the approach has an evidence base, and that it is appropriate for the participant's profile, strengthens the "likely to be effective" criterion.

Conclusion
Understanding the reasonable and necessary ndis framework is not just about compliance. It is about writing reports that genuinely reflect the functional impact of disability and make it easy for decision-makers to approve the supports your clients need.
The criteria are not designed to exclude people from the scheme. They are designed to ensure funding goes to supports that are appropriate, effective, and specific. When clinicians understand the framework and write to it, reports become clearer, decisions become faster, and participants get better outcomes.
If you are looking for tools to help structure your NDIS documentation, the NDIS report templates and wording resources in the PsychVault library are designed by clinicians for exactly this kind of work. They include functional impact wording prompts, justification frameworks, and structured report templates built around the reasonable and necessary criteria.
Discussion
Share your thoughts and experiences with this resource.
Sign in to leave a comment
Comments
Browse real clinician-designed resources
Move from strategy into implementation with templates, handouts, and psychoeducation tools already live on the marketplace.
Turn your own resources into a polished store
Publish clinician-grade templates, build trust signals, and start growing an evergreen library under your own brand.
Keep the topic cluster growing

A practical checklist for writing clearer NDIS psychology reports with stronger functional wording, cleaner recommendations, and less admin drag.
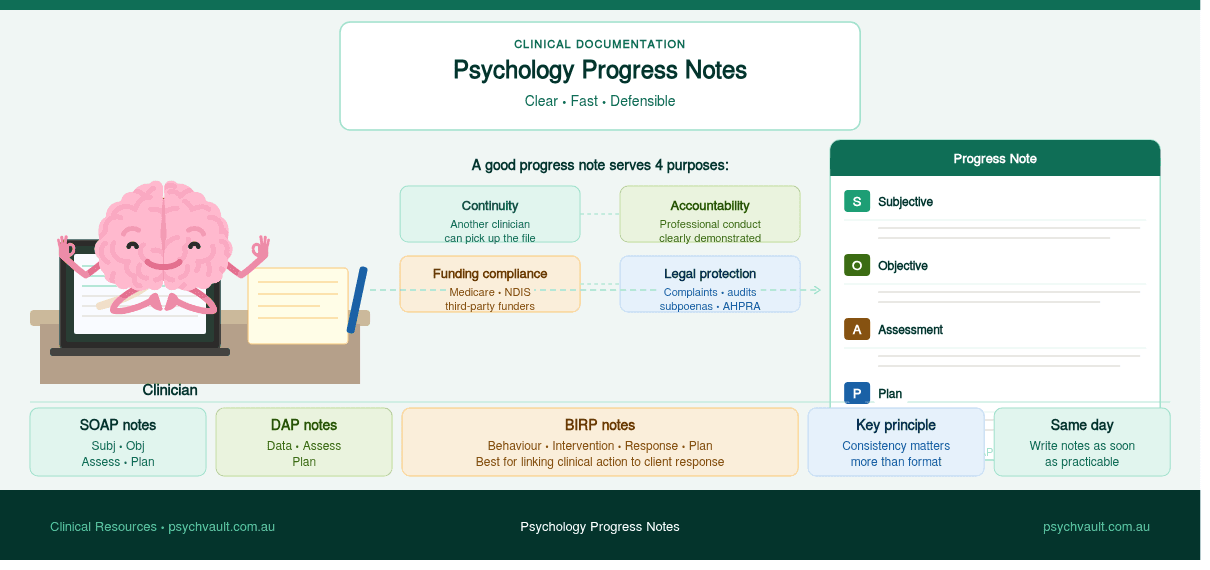
A practical guide for psychologists and clinicians on writing progress notes that satisfy clinical, legal, and funding requirements without turning documentation into a second full-time job.
A practical guide to the psychology templates clinicians use most — CBT worksheets, intake forms, case formulation, behaviour support, and NDIS documentation.