
How to write psychology progress notes that are clear, fast, and defensible
A practical guide for psychologists and clinicians on writing progress notes that satisfy clinical, legal, and funding requirements without turning documentation into a second full-time job.
Why progress note writing keeps getting harder
Progress notes are not new. Every clinician writes them. But for many psychologists, they remain one of the most time-consuming and anxiety-provoking parts of private practice.
The session ends. The next client is already waiting. There are three other notes from yesterday still unfinished. And somewhere in the back of your mind is the knowledge that whatever you write could appear in a subpoena, a Medicare audit, a NDIS plan review, or a complaint to AHPRA.
That combination of time pressure and legal exposure is why searches like psychology progress note template, how to write therapy notes fast, and what to include in a session note are so consistent. Clinicians are not looking for theory. They are looking for a structure that helps them document clearly, quickly, and defensibly — every session, every week.
This post provides exactly that.
What progress notes actually need to achieve
Before focusing on format, it is worth being clear about what a progress note is for.
A progress note is not a transcript of the session. It is not a detailed narrative of everything the client said. It is a clinical record that demonstrates what happened, why clinical decisions were made, and what comes next.
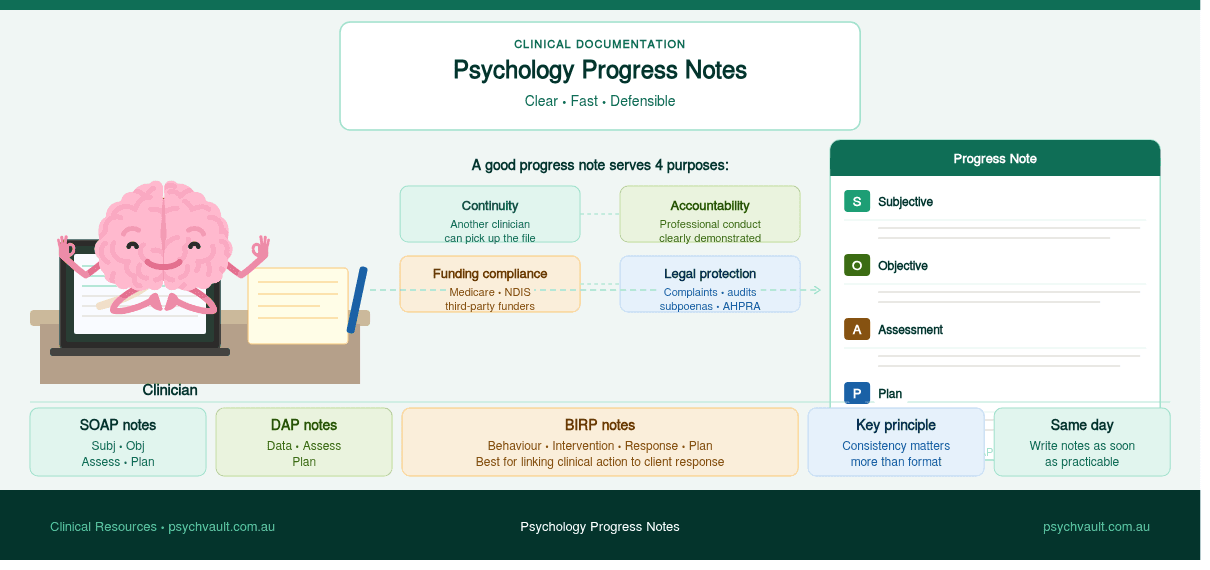
A well-written note should serve four purposes:
- 1Continuity of care — if another clinician picks up the file, they can understand where treatment stands
- 2Accountability — the note shows that you acted professionally and within your scope
- 3Funding and rebate compliance — for Medicare, NDIS, and third-party funders, the note is often evidence that the session occurred and was clinically appropriate
- 4Medico-legal protection — in complaints or legal proceedings, contemporaneous notes are your primary record
A note that satisfies all four purposes is not necessarily long. It is specific, structured, and clearly connected to treatment goals.
Choosing a progress note format
Several documentation frameworks are commonly used in psychology practice. The format you choose matters less than applying it consistently.

SOAP notes
SOAP is the most widely recognised format across health disciplines:
- S — Subjective: what the client reported (symptoms, experiences, mood ratings, significant events since last session)
- O — Objective: observable clinical information (affect, presentation, behaviour, relevant test results)
- A — Assessment: your clinical interpretation (how the client is tracking, any changes to formulation or risk)
- P — Plan: what was done in session and what happens next (intervention used, homework, referrals, next appointment)
SOAP works well because it separates what the client says from what you observe and interpret. This is particularly important for medico-legal purposes.
DAP notes
DAP is a simpler alternative that suits many psychology sessions:
- D — Data: everything observed and reported (combines S and O from SOAP)
- A — Assessment: clinical interpretation and progress
- P — Plan: session content and next steps
DAP is faster to write and often sufficient for straightforward therapy sessions with low complexity.
BIRP notes
BIRP is used in some mental health and community settings:
- B — Behaviour: what the client presented with
- I — Intervention: what you did clinically
- R — Response: how the client responded
- P — Plan: next steps
BIRP is particularly useful when you want to document the connection between your clinical action and the client's response.
Which format should you use?
Choose whichever structure fits your setting and patient population, and stick with it. Consistency matters more than format. A clinician who writes clear, consistent DAP notes will have a stronger record than one who switches formats session to session.
If you use a template, the format is largely handled for you. The real skill is in what you write inside the structure.
What to include in a psychology progress note
Regardless of format, strong progress notes tend to include the following elements.
Session identification
- Date, duration, and type of session (individual, couple, group, telehealth)
- Attending clinician and any supervision or consultation that occurred
Presenting state
A brief summary of how the client presented at the start of the session. This is not a verbatim account. It is your clinical observation of their mood, affect, and current situation.
Example: Client presented as fatigued and mildly dysphoric. Reported ongoing sleep disruption and a stressful workplace incident during the week. Affect consistent with reported mood. No observable distress at session commencement.
Risk screening
Every note should address risk, even briefly. If there are no concerns, say so explicitly. A note that is silent on risk creates an uncomfortable ambiguity if the record is ever reviewed.
Example: No suicidal ideation, self-harm, or risk to others reported or observed. Safety plan reviewed and remains in place.
Session content and intervention
What did you actually do in the session? This section should connect clearly to the treatment plan and the client's goals.
Example: Continued work on cognitive restructuring using CBT framework. Reviewed thought records completed between sessions. Identified three high-frequency automatic thoughts and examined evidence for and against each. Client demonstrated emerging ability to generate alternative appraisals with prompting.
Client response
How did the client engage with the material? Did they demonstrate understanding? Were there any difficulties?
Example: Client engaged well and noted that identifying the evidence for/against format was "more useful than she expected." Some difficulty generating alternatives in the moment; explored this as a target for practice before next session.
Plan
What is the clinical plan going forward? Include:
- Any between-session tasks
- Referrals or communications
- Next appointment details
- Any changes to treatment approach
Common progress note mistakes — and how to avoid them

Writing too much narrative
Notes that read like transcripts are harder to review, harder to search, and expose more information than necessary to third parties. Keep descriptions brief and clinical.
Writing too little
On the other end, notes like "session went well, CBT continued, client coping" are almost useless. They do not demonstrate clinical reasoning, document progress, or protect you legally.
Forgetting to address risk
Even a single sentence is sufficient if there are no concerns. Omitting it entirely creates a gap in the record.
Blurring fact and interpretation
Use clear language to separate what the client reported from your clinical interpretation. "Client reported feeling hopeless" is different from "client appears hopeless." Both may be true, but they are different clinical observations.
Documenting after a significant delay
Notes should be written as soon as practicable after the session — ideally on the same day. Delayed notes can be challenged in complaints and audits, and memory fades quickly in a busy caseload.
Using vague progress language
"Client is progressing well" means almost nothing without evidence. "Client demonstrated ability to apply distress tolerance skills independently during a high-stress week, consistent with treatment goal 2" says something real.
Progress notes for Medicare, NDIS, and private funders
If you are billing Medicare under a Mental Health Treatment Plan, your notes are part of the evidence trail that justifies the rebate. They should clearly show that you provided a psychological therapy session with appropriate clinical content, not just a supportive conversation.
For NDIS participants, progress notes often feed into plan reviews, reports to support coordinators, and evidence for ongoing therapeutic support funding. Notes that track functional progress over time — not just session content — are significantly more useful in those contexts.
If a funder or regulator can read your notes and understand what changed for the client and why your work contributed to that, the notes are doing their job.
For private health fund billing, consult your insurer's requirements. Some require specific wording or minimum content standards for session notes.
Telehealth progress notes
Telehealth sessions should be documented in the same way as in-person sessions, with two additions:
- 1Note the modality (e.g., video call via a specific platform)
- 2Note that the client consented to telehealth delivery for this session
This matters for Medicare compliance and medico-legal purposes. Some clinicians also note any technology difficulties that affected session delivery.
Using a progress note template in practice
A well-designed template is not a shortcut that reduces clinical thinking. It is a structure that ensures you capture the right information without having to reconstruct the format from memory after every session.
The best templates prompt you through each required section, leave enough space for real clinical content, and are formatted so the note reads logically whether it is reviewed on screen or printed.
PsychVault has a range of clinical documentation templates built specifically for Australian psychologists and allied health practitioners — including progress note templates formatted for different practice settings and client populations.
When evaluating any template, check that it covers:
- risk screening
- session content and intervention
- client response
- plan and next steps
- the relevant compliance elements for your billing context
A practical readiness check before you finalise a note

Before saving or submitting a progress note, run through this quick check:
- 1Does the note clearly describe how the client presented today?
- 2Is risk addressed, even briefly?
- 3Does the note show what clinical intervention occurred?
- 4Is there evidence of the client's response or engagement?
- 5Is the plan clear?
- 6Could another clinician pick up this file and understand where treatment stands?
- 7Does the note avoid over-sharing information the client would not expect to be documented?
If yes to all seven, the note is doing its job.
Final thoughts
Progress notes are not paperwork to get through as fast as possible. They are part of professional practice, legal protection, and continuity of care.
The goal is not to write long notes. It is to write notes that are clear, specific, and clinically grounded — notes that demonstrate your thinking without becoming a burden on the rest of your day.
A reliable structure, a good template, and a consistent habit of writing same-day notes will take most of the cognitive drag out of this part of practice. What remains is the actual clinical reasoning — which is the part worth spending time on.
Discussion
Share your thoughts and experiences with this resource.
Sign in to leave a comment
Comments
Browse real clinician-designed resources
Move from strategy into implementation with templates, handouts, and psychoeducation tools already live on the marketplace.
Turn your own resources into a polished store
Publish clinician-grade templates, build trust signals, and start growing an evergreen library under your own brand.
Keep the topic cluster growing
A practical guide to the psychology templates clinicians use most — CBT worksheets, intake forms, case formulation, behaviour support, and NDIS documentation.

A practical checklist for writing clearer NDIS psychology reports with stronger functional wording, cleaner recommendations, and less admin drag.

Understand the NDIS reasonable and necessary criteria and learn how to write reports that justify supports clearly, specifically, and effectively.