
What Are Neuroaffirming Templates — And Why Do They Look Different From Standard Clinical Resources?
A practical guide for Australian psychologists and allied health clinicians on what neuroaffirming documentation actually means, and how to spot it in the resources you use.
There is a version of neuroaffirming practice that lives entirely in theory.
It shows up in professional development slides, in position statements, in the language clinicians use to describe their approach on their website. It sounds right. But it does not always make it onto the page — the actual page, the one a client picks up at the start of their first appointment.
That is where templates come in. And it is where a lot of otherwise well-intentioned clinical practice quietly slips back into old habits.
This post is about what neuroaffirming documentation actually looks like in practice, why standard clinical templates can work against the goals of affirming care, and what to look for when you are choosing or designing resources for your clinic.
Jump to a section:
- Why documentation is part of the clinical relationship
- What changed in December 2025
- What makes a template neuroaffirming — and what does not
- How it shows up differently across template types
- The practical question: do your current templates pass?
- Where to find neuroaffirming templates built for Australian clinicians
Why documentation is part of the clinical relationship
Most clinicians think about neuroaffirming practice in terms of what happens in the room. How they communicate. How they structure sessions. Whether they allow movement, accommodate sensory needs, follow the client's lead on communication style.
All of that matters. But the documentation a client encounters before, during, and after the clinical encounter is also doing something. It is signalling how you see them.
An intake form that asks a client to list their "deficits" or "problem behaviours" before you have even met is already framing the relationship in a particular way. A goal-setting worksheet that positions the client as someone who needs to be fixed, rather than someone who is trying to navigate a world that was not built for them, is doing the same thing.
For neurodivergent clients, many of whom have spent years being assessed, categorised, and managed by systems that pathologised their natural way of being, this matters more than it might seem. The language on the page is not neutral. It tells them what kind of clinician you are, before you say a word.
This does not mean clinical documentation needs to be stripped of clinical content. Good neuroaffirming templates are still rigorous. They still capture the information you need for assessment, treatment planning, and reporting. They just do it from a different starting point.

What changed in December 2025
In December 2025, the Psychology Board of Australia updated the core competency standards required for general registration. For the first time, neurodiversity-informed practice was included as an explicit professional standard — not a specialisation, not an optional CPD category, but a baseline expectation for every registered psychologist in Australia. Competency 7.9 specifically requires that psychologists understand neurodiversity, strengths-based and trauma-informed approaches, and can adapt their practice and make reasonable adjustments for people with disability.
This is a meaningful shift. It means neurodiversity-affirming practice is now part of what it means to practise ethically and competently. A forensic psychologist, a school psychologist, a clinician in private practice — all are now professionally accountable for practising in a way that is informed by an understanding of neurodiversity.
The practical implications of this are still being worked through. But one clear implication is that the tools clinicians use — including templates, handouts, worksheets, and psychoeducation resources — need to reflect the same values that the competency standards describe.
If your intake form still describes autism as a disorder characterised by deficits in social functioning, your templates are out of step with your professional obligations.
What makes a template neuroaffirming — and what does not
The differences between a standard clinical template and a neuroaffirming one are not always obvious at first glance. They often come down to framing, language, and structure rather than dramatic visual or content differences.
Here is what to look for.
Language that starts from difference, not deficit
Standard clinical language tends to describe neurodivergent traits in terms of what is absent or impaired. Neuroaffirming language describes the same traits in terms of difference — a genuine variation in how someone thinks, processes, and experiences the world, with both strengths and challenges. One rule of thumb Behaviour is communication and people communicate differently and thats okay.
This is not about avoiding clinical accuracy. It is about recognising that the words used to describe someone's neurodivergence shape how they understand themselves. Avoid potential shameful lanague - A client who has spent years being told they have "poor social skills" and "restricted interests" experiences their neurodivergence differently to one whose intake form asks about their communication preferences and areas of deep engagement.
Both describe the same person. Only one is affirming.
Strengths as a genuine section, not a courtesy field
Many standard templates include a strengths section as an afterthought — a single line at the bottom of a page dominated by problem areas. Neuroaffirming templates treat strengths as clinically significant information, not a checkbox.
This matters for assessment, for treatment planning, and for the client's experience of the process. A formulation that integrates a client's strengths is a better clinical document than one that only maps difficulties. It is also a more accurate one.
Flexible format and response options
Standard templates often assume a single mode of engagement — written responses, in full sentences, within a fixed space. For many neurodivergent clients, this format is a barrier rather than a tool.
Neuroaffirming templates account for this. They might offer multiple ways to respond to the same question. They leave enough space for different communication styles. They do not penalise brevity or non-linear thinking. They avoid jargon that assumes a particular educational background or familiarity with clinical language.
Communication and sensory preferences built into the intake process
A neuroaffirming intake form does not wait until something goes wrong to ask about a client's access needs. It asks upfront: how do you communicate best? Are there sensory considerations we should know about? Do you prefer written communication between sessions? Is there anything about this environment that would make it harder or easier for you to engage?
These questions are not administrative. They are clinical. They tell you something important about how to work effectively with the person in front of you. Templates that include them are doing more clinical work than templates that skip them.
Goals framed around the client's own priorities
Standard goal-setting frameworks often work from a treatment goal — a clinical target the clinician has identified as the focus of intervention. Neuroaffirming goal-setting starts somewhere different: what does the client actually want? What would a good life look like to them, in their terms?
This is not always the same thing. And for neurodivergent clients, the gap between "what the clinician thinks should change" and "what the client actually wants" can be significant. Templates that build in co-defined goals, that ask the client to articulate what matters to them before any clinical framework is applied, are doing something genuinely different.
How it shows up differently across template types
Neuroaffirming principles do not look the same across every type of clinical resource. Here is a brief breakdown of what to look for in each.
Intake and assessment forms
The most important changes are in language and question framing. Deficit-led language should be replaced with difference-led language. Communication preference fields should be included. There should be space for the client to describe how they experience their neurodivergence in their own words, not just respond to a list of clinical descriptors.
Assessment forms used with children or young people carry additional responsibility. The way a young person's profile is described in the assessment process shapes how parents, teachers, and the young person themselves understand that profile for years. Forms that describe a child as "lacking" something are doing harm the clinician may not intend.
Psychoeducation handouts
Psychoeducation resources are often where the most unreconstructed deficit-model language persists. Handouts about autism, ADHD, or other neurotypes that were written ten years ago frequently describe these as disorders defined by what the person cannot do.
Neuroaffirming psychoeducation reframes this. It explains the neurotype in terms of how the person's brain works differently, what environments and conditions support them, and what challenges arise specifically from the mismatch between their neurotype and a world that was designed around neurotypical norms. That framing is both more accurate and more useful for the person trying to understand themselves.
Goal-setting and treatment planning worksheets
The key shift here is from clinician-led to genuinely collaborative. Neuroaffirming goal-setting worksheets create space for the client to identify their own priorities before any clinical framework is introduced. They separate "what I want for my life" from "what we will work on in sessions" in a way that respects client autonomy.
They also avoid language that positions the goal as eliminating or reducing a neurodivergent trait. Reducing a client's stimming because it makes other people uncomfortable is not an affirming goal. Supporting a client to develop strategies that give them more choice over how and when they stim is a different thing entirely.
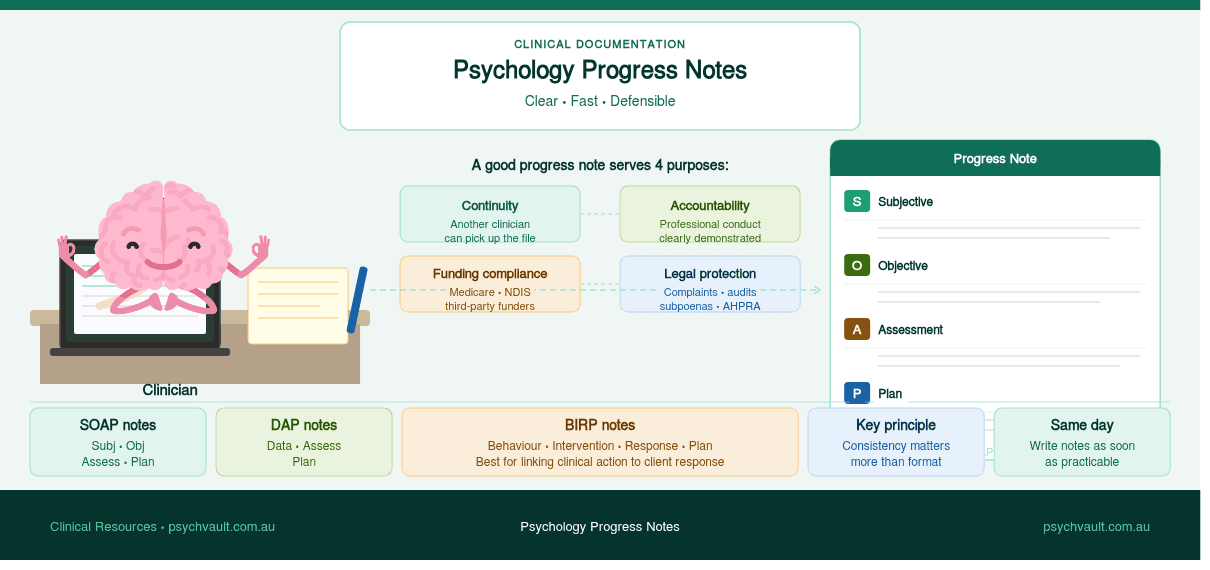
Progress notes and clinical summaries
Progress notes are less often discussed in the context of neuroaffirming practice, but they matter. Notes that consistently describe a neurodivergent client's presentation in deficit terms contribute to a cumulative clinical record that shapes how every future clinician who reads that file sees that person.
Neuroaffirming progress notes describe what the client did, what they engaged with, and how they responded — not what they failed to do. They track functional progress in the client's own terms, not just against external benchmarks.
The practical question: do your current templates pass?
It is worth sitting with that question genuinely, rather than assuming the answer.

Most clinicians working in Australia right now trained in a period when the deficit model was the standard framework. The templates many of us still use were designed in that context. They are not necessarily bad resources — but they were not designed with neurodiversity-affirming practice in mind, and it shows.
A quick audit of your current intake form is a useful starting point. Read it as if you are a neurodivergent adult attending their first psychology appointment, carrying years of experiences of being assessed, categorised, and told what is wrong with you. What does the form communicate about how this clinician sees you?
If the answer is uncomfortable, that is useful information.
The goal is not to throw out clinical rigour. It is to apply that rigour from a starting point that treats neurodivergent ways of being as legitimate variations in human experience, rather than problems to be corrected.
Where to find neuroaffirming templates built for Australian clinicians
Adapting existing templates is one option. But it is time-consuming, and the results are inconsistent — particularly when the original template was built on a framework that is fundamentally at odds with neuroaffirming practice. Patching deficit-model language is not the same as starting from an affirming framework.
PsychVault's neuroaffirming template range has been built from the ground up by practising Australian clinicians for use in real clinical settings. That means the language, structure, and clinical content reflect current best practice, not a retrofitted version of an older model.
The range includes intake and consent documentation, psychoeducation resources for common neurotypes, goal-setting and treatment planning tools, and progress note frameworks — all designed to work together and all written for the Australian clinical context.
Browse neuroaffirming templates on PsychVault
A note on language
Neuroaffirming practice includes being thoughtful about the specific language used to describe neurodivergent identities. Within autistic communities in particular, there is ongoing discussion about identity-first versus person-first language — "autistic person" versus "person with autism."
Research and community consultation consistently finds that the majority of autistic adults prefer identity-first language, viewing autism as a core part of their identity rather than something separate from the person. This preference is not universal, and the most affirming approach is always to follow the individual client's lead on how they describe themselves.
Where possible, templates should be designed to accommodate both, and clinicians should not assume a preference without asking.
PsychVault is a marketplace for psychology and allied health resources designed for real clinical work. All resources are created by practising Australian clinicians. Browse the full range here.
Discussion
Share your thoughts and experiences with this resource.
Sign in to leave a comment
Comments
Browse real clinician-designed resources
Move from strategy into implementation with templates, handouts, and psychoeducation tools already live on the marketplace.
Turn your own resources into a polished store
Publish clinician-grade templates, build trust signals, and start growing an evergreen library under your own brand.
Keep the topic cluster growing

A practical guide to creating psychoeducation handouts for Australian practice — clear, credible, and designed for real clinical sessions.
A practical guide for psychologists and clinicians on writing progress notes that satisfy clinical, legal, and funding requirements without turning documentation into a second full-time job.

A practical checklist for writing clearer NDIS psychology reports — stronger functional wording, cleaner recommendations, and less admin for Australian clinicians.